Howard Tayler posts reviews of movies he has viewed, and a common thread in the movies deals with the visual effects of 3-D and "shaky cam." The problems with these film-making techniques are numerous - yet, they can all be accounted for by examining how the visual system processes and interprets the information.
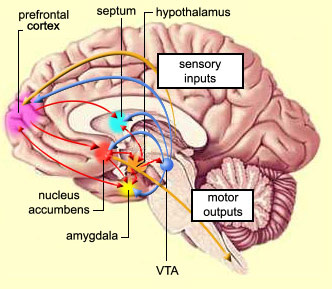
Referring to the diagram at right, we see the primary visual pathway, where visual information transfers from the retina to the Thalamus (lateral geniculate nucleus) to the primary visual cortex in the Occipital Lobe (by the way - three cheers to Howard Tayler - he is a writer who "gets it right!"). As an object moves across our field of view, clearly it will activate different regions of visual cortex, and hence the motion will be perceived in our visual processing. In fact, there is a controversial hypothesis that states that output from the visual cortical regions follows two pathways - one to the temporal lobe to be combined with memory and identify "what," and the other to parietal lobe to be combined with sensory and motion information and identify "where."
However, this "well-known" aspect of visual processing ignores an important, lower pathway by which visual information is processed. See the yellow "buttons" in the diagram labeled "Superior Colliculus?" Also, note that there is no indication of visual information projecting to the Cerebellum? Well, this often neglected pathway directly processes visual motion, and is necessary to keep the eyes pointed at moving objects - in other words, motion tracking. Neurons in lateral geniculate also project to Superior Colliculus (SC) and Cerebellum. Neurons in Cerebellum in turn project back to the SC and the Frontal Eye Fields in the Frontal Lobe. Frontal Eye Fields then project to the Occulomotor Nucleus which controls the Occulomotor nerve for control of eye position, and the Locus Coeruleus ("blue nucleus") and Edinger-Westphal Nucleus which affect the pupil and lens of the eye to regulate focus and amount of light reaching the retina. Superior Colliculus and Occulomotor nerve are part of what is termed the "optic tectum" in the mesencephalon, or midbrain.

So, what does this have to do with 3-D and "shaky cam?" Well, lets look at what also connects with the same midbrain areas:
The diagram at left shows the human brainstem, and immediately below the SC, we see the Inferior Colliculus (IC). IC serves a similar function to the SC, except for the auditory system. IC and several smaller nuclei referred to as the Superior and Inferior Olive - or Olivary Complex - participate in tracking moving sound. In particular, the Olivary complex compares the timing of sounds from both ears to localize the source of the sound from right to left. IC communicates with the vestibular ("Semicircular Canals" - balance system in the inner ear), and with the Cerebellum (as does the Olivary Complex) to coordinate motor commands to move the eyes to complete the tracking of a moving sound. But just as important are the nuclei located in the same part of the midbrain - the Raphe Nuclei. Neurons in these nuclei utilize Serotonin as a neurotransmitter. The nuclei have various functions in attention, circadian rhythm, motor coordination, overall brain activation, depression, pain sensation and hallucination. The dorsal Nucleus Linearis and Dorsa/Medial Raphe are sensitive to hallucinogens such as LSD. The medial nuclei in the Pons are connected to the cerebellum for motor learning and coordination, while the ventral nuclei in medulla regulate pain sensation, fever, respiration, heart rate and contractions of the stomach and intestines (related to nausea). There are interconnections between all of the areas - through the optic tectum, Cerebellum and Spinal Cord as well as direct interconnections.
Thus we see that the visual motion system is interconnected with systems that perceive balance and control the brains awareness of its position with respect to moving sights and sounds. It is indirectly connected with brain areas that regulate bodily functions such as pain sensation, heart rate and nausea. Thus what a "good" 3-D visual experience does is to provide what viewers would consider a more *visceral* experience - *precisely* because it activates additional brain systems that fool the body into experiencing more sensation than just the visual.
And herein lies the problem.
The mismatch between what the eyes see, the ears hear, and the feedback from the rest of the body is a problem for the brain. "Shaky cam" gives the sensation of normal body movement - as a person moves through their environment, the point of view continually moves - shakes, turns, rotates back-and-forth - but the brain DOES NOT PERCEIVE THAT MOTION! Proprioceptive feedback from the body, Cerebellar interactions with the occulomotor system, and the decades of learned experience lead the brain to perceive a steady, continuous view of the environment - in fact, *memory* of previous views allow us to have a perception of our entire surroundings, even when we aren't actually looking at them. "Shaky cam" violates that perception. We don't have the feedback from muscle movements to allow the brain to correct for the motion, and it makes us feel uncomfortable.
Sometimes that the point - "The Blair Witch Project" and "Cloverfield" used the "shaky cam" precisely to make the audience uncomfortable. However, that trick only works a few times, it is best used sparingly, and has no place in a movie with the intent to entertain without a brooding, disturbing background. Thus, any other use of "shaky cam" is just inappropriate and shoddy film-making. It leaves the audience with headaches and nausea, and -yes- feeling like they've just had a bad LSD trip. It is a gimmick, a trick used by producers and directors to be "trendy" but just reflects poorly on their own skills.
The visual system does not actually require 3-D effects (and really *cheesy* ones at that!) to perceive the three dimensional aspects of a scene. The visual association areas in the Parietal Lobe compare many aspects of a scene to provide knowledge of depth and perspective - for example, a small object, moving slowly across the scene is perceived as being further away than a large object moving quickly. Eclipsing of an object, where one object is covered by another, is perceived as the disappearing object being *behind* the still-visible object. Objects which get larger are perceived as coming toward the viewer, while objects getting smaller are perceived as moving away.
After all, stereoscopic vision relies on two eyes placed 7-8 centimeters apart. Once an object is more than 100 times that distance away (call it 10 meters distant), there is *very little* stereoscopic difference. Add to that the problem of corrective eyeglasses - correction of nearsightedness requires eyeglass lenses that make an object smaller in the course of correcting the focus. When a person has two eyes requiring different correction, the brain has to resolve two different sized images projected onto retina. Three-dimensional interpretation of our environment essentially requires a *lot* of processing involving visual and association cortex, the processing nuclei and Cerebellum - but mostly the visual association areas.
This is not to say that 3-D TV and movies don't have their place. There is an incredible feeling - again, a "visceral" one - of viewing a 3-D film. But in reality, that sensation is also gained by very high resolution, large-screen HDTVs and in IMAX theaters, so that the visual system can clearly see all the details that it uses to construct the three-dimensional perception. The feeling of immersion is assisted by 3-D audio effects as well. But over-use of 3-D - that is, over-stimulation by 3-D - results in headaches and nausea, precisely because it elicits that "gut-reaction" to the visual images. The aforementioned eyeglass wearers might *never* have a comfortable 3-D experience because of visual mismatch. Let us not forget that the mismatch also extends to the difference between the visual system and the body - with the visual and auditory system telling the brain that the body should be moving, at the same time that the body is telling the brain that it is *not* moving!
Use of 3-D - in the flying sequences of "How to Train Your Dragon" - yes, thumbs up! To "Toy Story," "Journey to the Center of the Earth," and "Thor" - no, thumbs down.
To directors and filmmakers: Stop using cheesy effects because you don't have the skills to make a better movie. *Learn* some brain science and GET IT RIGHT! and stop giving us headaches and making us sick to our stomachs!
Tune in to The Lab Rats' Guide to the Brain for more on how to "get it right" in brain science ... after all, it's not brain surgery...